If you’re considering upper jaw all on 4, you’ve probably heard two things at once: It’s possible, and the upper jaw is trickier. Both can be true. The upper jaw often has softer bone and sits next to the maxillary sinuses, which can limit implant placement and affect “same-day teeth” decisions.
This guide, by Prof Clinic Istanbul, for patients considering upper jaw All-on-4 in Turkey, aims to explain why the upper arch is different, what your CBCT scan is really checking for, and how clinicians choose between standard All-on-4, modified implant numbers, grafting, or advanced options like zygomatic implants, without hype or guarantees.
This article is for education and does not replace an in-person exam. Implant candidacy and timing depend on your anatomy, medical history, bite forces, and clinician judgment.
Why is upper jaw all-on-4 often more challenging than lower jaw?
Maxillary all on 4 can be more complex than lower-jaw full-arch work for two main reasons:
- Bone quality: The top teeth often have a higher proportion of spongy bone and thinner outer cortical bone. That can make it harder to achieve primary stability.
- Sinus anatomy: The maxillary sinuses sit above your back upper teeth. After tooth loss, the sinus can expand downward, and the ridge can shrink, leaving less vertical bone for posterior implants.
If you want the bigger picture first, see our Full Arch Dental Implants blog, then come back here for the maxilla-specific details.
Why Is Bone Quality Different in the Upper Jaw?
Think of jawbone like building material:
- Cortical bone offers stronger initial mechanical anchorage.
- Trabecular bone can be excellent bone biologically, but may provide less immediate grip, especially when bone volume is reduced.
The upper jaw often has less dense bone than the lower jaw, so it may need to use strategies that improve stability. This is one reason “same-day teeth” is case-dependent in maxillary all on 4.

Bone Density & Primary Stability in the Upper Jaw
Primary stability is the immediate tightness of the implant in bone. Osseointegration is the longer biological bonding process that happens during healing. In softer maxillary bone, primary stability can be more variable, which affects whether immediate loading is a safe call.
High survival for All-on-4 overall is generally shown, but some cohorts report the maxilla as a higher-risk arch compared with the mandible, particularly for early failures, highlighting why careful selection and loading protocols matter.
What clinicians may adjust in softer upper bone without promising a one-size-fits-all outcome:
- Implant positioning to maximize bone contact in stronger zones (often anterior maxilla).
- Implant distribution (A-P spread) to reduce cantilevers.
- Tilted posterior implants to avoid the sinus and improve anchorage/distribution in available bone.
- Loading decisions (fixed temporary vs delayed loading) based on stability and bite conditions rather than marketing terms like “guaranteed teeth in a day.
If you want context on implant designs/materials without getting lost in brand hype, see our blog about types of dental implants.
Contact us via WhatsApp to ask for a plan that states whether immediate fixed temporary teeth are recommended for your upper arch and why. At Prof Clinic, we can guide this through an online assessment workflow.
How does Poor bone density affect implant stability and healing time?
When bone is softer or thinner:
- Clinicians may be more conservative with bite forces during early healing (soft diet, careful chewing guidance).
- The temporary bridge may be designed to reduce load (e.g., controlled occlusion, reduced cantilever).
- Follow-ups matter more: hygiene, inflammation control, and bite adjustments can protect integration.
In other words, healing can still be smooth, but the plan often prioritizes risk reduction over speed.
How does maxillary sinus affect implant placement?
The maxillary sinus is an air-filled cavity lined by a thin membrane. After upper back teeth are lost, two changes commonly happen:
- The ridge can resorb (bone loss).
- The sinus can expand downward (pneumatization).
Both can reduce available bone height for posterior implants, increasing the importance of CBCT-based planning and careful angulation.
Sinus-related concerns in upper jaw All-on-4 planning often include:
- Residual bone height under the sinus
- Sinus membrane thickness
- History of chronic sinus issues
- Risk of membrane perforation during sinus-related procedures
For the All-on-4 basics, see All-on-4 Guide; this article stays focused on maxilla-specific issues.
Can sinus infections increase the risk of implant complications?
Active sinus disease should be evaluated before elective upper-jaw implant surgery. The goal isn’t to disqualify you; it’s to reduce preventable risk by clarifying whether inflammation, obstruction, or infection needs ENT/dental coordination first.
Pre-op assessment and understanding sinus pathology are repeatedly emphasized in sinus elevation literature.
What is the risk of sinus perforation during upper jaw implant placement?
Sinus membrane perforation is a recognized intraoperative complication in sinus augmentation procedures and can influence postoperative healing depending on size and management.
Prevention and management strategies are discussed in clinical reviews of sinus augmentation complications.
Sinus Lift & Bone Grafting: When It’s Needed?
All-on-4 was developed, in part, to reduce the need for extensive grafting by using available anterior bone and tilting posterior implants to avoid anatomical limits like the sinus. But reduce is not the same as never.
Below is a simplified table showing how CBCT findings often guide options. This is not a substitute for a clinician’s plan; it’s a way to understand the logic.
| Upper-jaw CBCT finding | What it usually means |
| Adequate anterior bone; sinus limits posterior height | Graftless may be realistic if stability and distribution are achievable |
| Limited residual bone under sinus in posterior region | Posterior anchorage may be constrained |
| Severe maxillary resorption and unfavorable sinus anatomy | Standard All-on-4 may not provide predictable support spread |
| Signs of active sinus disease / unresolved chronic symptoms | Higher risk environment for sinus procedures |
A sinus lift creates more vertical bone height in the posterior maxilla. It can be done via a window approach or a transcrestal approach, depending on anatomy and goals. Both techniques and their complications are described in clinical overviews
If you want clarity, schedule your consultation to discuss your plan that compares standard/modified All-on-4 vs grafting/sinus work vs advanced anchorage options based on your CBCT.
Can severe maxillary bone resorption be treated with standard All-on-4?
Sometimes, but not always predictably.
Severe resorption can reduce:
- the ability to spread implants for stability,
- posterior support (because of sinus limits),
- and the safety margin around vital anatomy.
In these cases, teams may recommend more implants, a different distribution, staged augmentation, or an advanced approach because the goal is not fewest implants, it’s a stable, maintainable result matched to your anatomy.
For a comparison of when more implants may be considered, see All-on-4 vs All-on-6
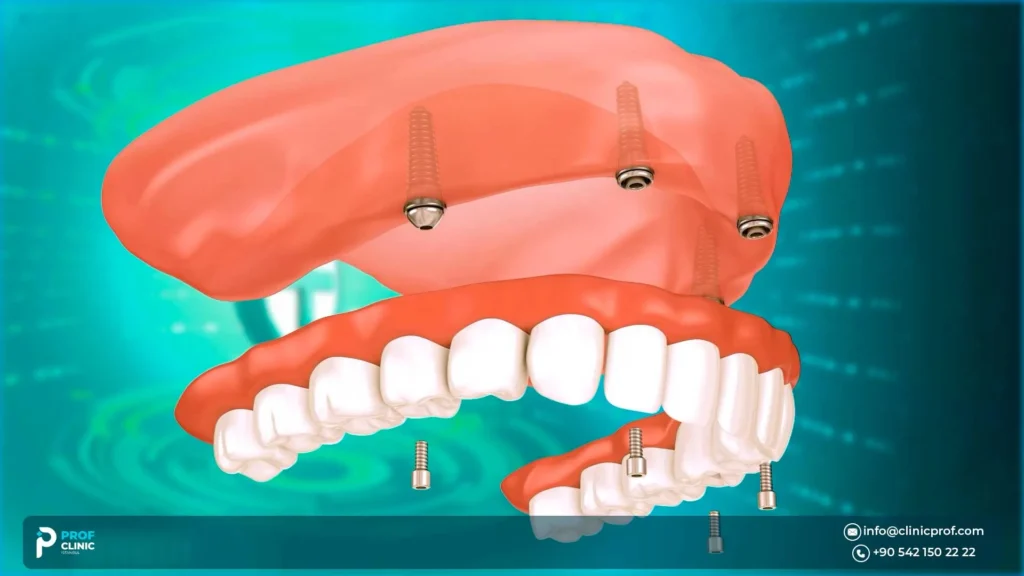
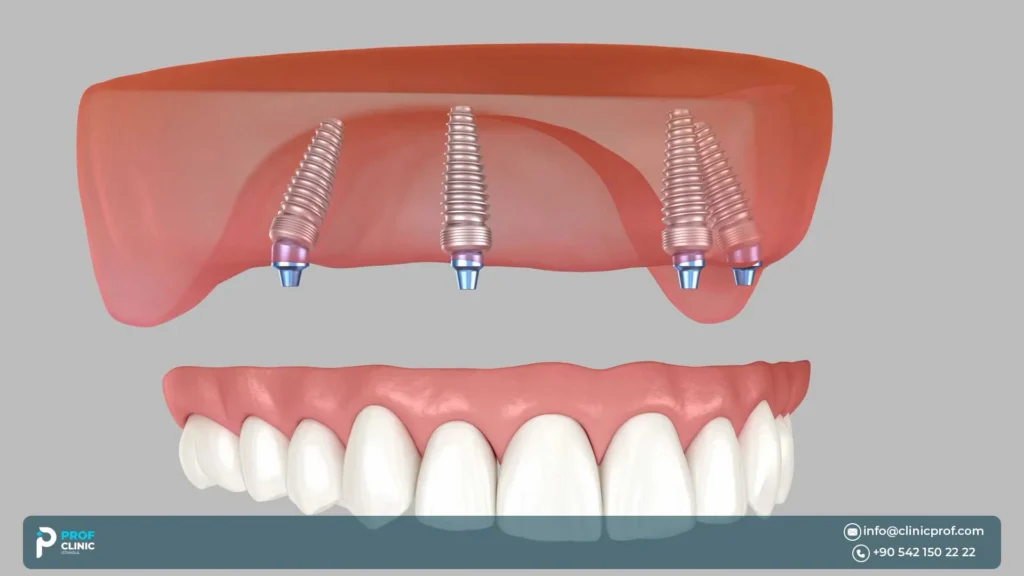
Implant Angulation in the Upper Jaw
Tilted posterior implants are commonly used in All-on-4 planning to:
- avoid the sinus (and other anatomical limits),
- increase the A-P spread (reducing cantilever),
- improve distribution along the arch.
Why tooth position matters
In upper-arch cases, aesthetics and speech are tightly linked to tooth position. Prosthetic-first means the team plans:
- where teeth should sit for smile line and lip support,
- where the screw-access should emerge,
- Then places implants to support that plan safely.
This approach is especially helpful in the maxilla, where sinus and bone constraints can push implants off “ideal” positions unless the plan is coordinated from the start.
If you’re exploring immediate temporary teeth timing, see Same-Day All-on-4: Teeth in One Day Possible?
Does the Upper Jaw Require Longer Implants for Better Anchorage?
Sometimes—but not as a universal rule.
Implant length is limited by available bone and proximity to the sinus. Stability comes from a combination of:
- bone quality and quantity,
- implant design and placement technique,
- and the planned bite forces and prosthesis design.
A “longer is always better” mindset can be misleading in the upper jaw, because anatomy sets boundaries—and safety matters.
When zygomatic implants or other advanced options are considered?
When the upper jaw is severely resorbed and sinus anatomy limits conventional posterior implants, zygomatic implants can be an alternative. These anchor into the zygomatic (cheek) bone to support a fixed full-arch prosthesis—often avoiding large grafting procedures in selected cases.
- Zygomatic implants are advanced and technique-sensitive.
- They can be part of a hybrid plan, depending on anatomy and surgical judgment.
- Indications and outcomes are discussed in consensus reports and systematic reviews.
| Pathway | why | Trade-offs to understand |
| Standard/modified All-on-4 | When anatomy allows stable distribution without extensive augmentation | May require cautious immediate loading criteria in soft bone |
| All-on-6 (or more implants) | When additional support/distribution is preferred in softer bone or higher forces | More implant sites; planning still must respect sinus limits |
| Zygomatic pathway | Severe maxillary atrophy where conventional posterior implants aren’t feasible | Advanced surgery; sinus-related complications can occur; requires experienced team |
What happens if there is severe bone loss in the upper jaw?
A realistic set of options your provider may discuss:
- More implants to improve support.
- Bone grafting when anatomy supports predictable augmentation.
- Zygomatic implants or hybrid solutions for severe atrophy, especially when avoiding staged grafting is a priority.
If you’re evaluating medical travel, contact us for a plan that includes what follow-up looks like after you return home
Complications to upper jaw all-on-4 and how they’re managed?
Every surgery has risks. Upper-jaw All-on-4 has some themes that are more maxilla-specific:
- Sinus-related events: membrane perforation during sinus augmentation (if performed), postoperative sinus symptoms, sinusitis risk in susceptible patients.
- Bone density sensitivity: softer bone can increase vulnerability to early failures if loading is too aggressive or stability is insufficient.
- Prosthetic biomechanical issues: excessive cantilever, poor distribution, or unbalanced bite forces can stress implants or the temporary bridge.
- Hygiene access under the bridge: upper-arch contours and tissue thickness can make under-bridge cleaning essential.
For prosthesis expectations and hygiene realities, see our blog titled Fixed vs Removable Implant Dentures
How stable are implants in the upper jaw?
Implants can be very stable in the upper jaw when the plan matches anatomy. Risk is influenced by:
- Anatomy: bone quality/volume, sinus constraints.
- Loading protocol: immediate vs delayed, provisional design, bite scheme.
- Patient factors: smoking, diabetes control, bruxism/clenching, oral hygiene, previous infections.
A helpful way to think about it: your provider can’t will stability into existence, but they can measure, plan, and choose a safer pathway when conditions are borderline.
How Do Doctors Plan Upper Jaw All-on-4 in Turkey?
Upper-jaw planning is where the best teams slow down and get specific. A typical safety-first workflow includes:
- Clinical exam and bite analysis, including clenching habits and wear patterns
- CBCT imaging to map bone volume, sinus anatomy, and critical structures
- Prosthetic-first planning to set tooth position for smile line, lip support, and phonetics
- Surgical planning for implant distribution, angulation, and safety margins
- Loading decision, based on stability and occlusal risk management
CBCT is consistently described as crucial for preoperative assessment in maxillary implant planning because it helps identify anatomical landmarks and indications for bone augmentation while minimizing surgical risks.
Bring this to your consult:
- Do I need a CBCT, and will you review sinus anatomy and pathology?
- What is your prosthetic plan first (smile line, lip support, speech contours) before implant placement?
- How will you decide fixed temporary teeth vs delayed loading for my upper arch?
- How will you control cantilever and bite forces in the provisional?
- If my bone is limited, what is the comparison between:
- modified All-on-4,
- All-on-6 (or additional implants),
- sinus lift/grafting,
- and zygomatic options if indicated?
- What is the maintenance plan (cleaning tools, recall schedule, bite checks)?
For trust and team transparency, see our Medical Team. You can also view our Testimonials for patient experience context.
Schedule your consultation and request a step-by-step upper-jaw plan
Also read: Same-Day All-on-4: Teeth in One Day Possible?
Recovery, Speech, Aesthetics & Same-Day Teeth in Istanbul
Upper-arch recovery is often described as manageable, but it can feel different than lower-arch work because the upper jaw involves:
- more visible aesthetics (smile line, lip support),
- speech-sensitive contours (palate/lingual surfaces),
- and (in some patients) sinus proximity considerations.
What does recovery often involve?
- Swelling and soreness for a short period after surgery
- Diet progression from soft foods to more normal chewing as directed.
- Hygiene routines under a fixed provisional bridge and around implant sites.
- Follow-ups to adjust bite and check tissue healing.
If you’re searching for top teeth implants specifically, the upper arch is where speech and smile line changes are most noticeable, so a careful temporary bridge design and patient adaptation period matter.
Same day typically means a fixed temporary bridge placed soon after surgery only if stability and bite conditions are met; it’s not automatic in every maxilla case.
A deeper explanation of temporary vs final timing is on Same-Day All-on-4
If you’re traveling to Istanbul, Turkey for treatment, ask for a written timeline of visits, temporary-teeth stages, and when follow-up checks should happen before you fly home.
Our full-arch overview emphasizes expectation-setting around temporary vs final teeth.
Are temporary dentures needed before final teeth?
Often, you’ll have some form of temporary teeth while implants integrate:
- Fixed temporary bridge (commonly used when immediate loading criteria are met).
- Removable temporary (used when stability is not sufficient for fixed immediate loading, or when tissue healing needs more protection).
The “best” option depends on stability, bite, and how the temporary will distribute forces during healing.
FAQs about upper jaw all on 4
What is the success rate of All-on-4 in the upper jaw?
Studies generally report high survival for All-on-4 overall, but results vary by follow-up duration, patient factors, and technique. A long-term cohort with 3–17 years of follow-up found high survival in both arches while reporting the maxilla as a risk factor with slightly lower cumulative survival than the mandible in that population.
How Long Does Upper Jaw All-on-4 Surgery Take in Turkey?
It depends on extractions, bone conditions, and whether additional procedures are required (sinus-related work, grafting, or advanced options). Your surgeon can estimate timing after CBCT review and medical history evaluation.
Is swelling worse in upper jaw All-on-4?
Swelling varies by individual. Upper-jaw procedures can feel different due to soft tissue and, in some cases, sinus proximity. Good planning and aftercare typically keep discomfort manageable, but expectations should be individualized.
Can I Get Same-Day Teeth for the Upper Jaw in Turkey?
Sometimes. “Same-day teeth” usually refers to a fixed temporary bridge delivered soon after surgery when stability and bite conditions allow—it is not guaranteed for every maxilla.
How long before I can eat normally after upper jaw surgery?
Most patients progress gradually from soft foods to more normal chewing based on stability, healing response, and your provider’s staged diet instructions. Early overload is a known risk, so follow your plan closely.
Can upper jaw All-on-4 fail more often?
Yes, it can be slightly higher risk than the lower jaw in some studies—mainly because the upper jaw often has softer bone and sinus-related limits, which can make early stability more sensitive. That said, overall All-on-4 survival is generally high when case selection, CBCT planning, and loading protocols are done properly, like we did at Prof Clinic.
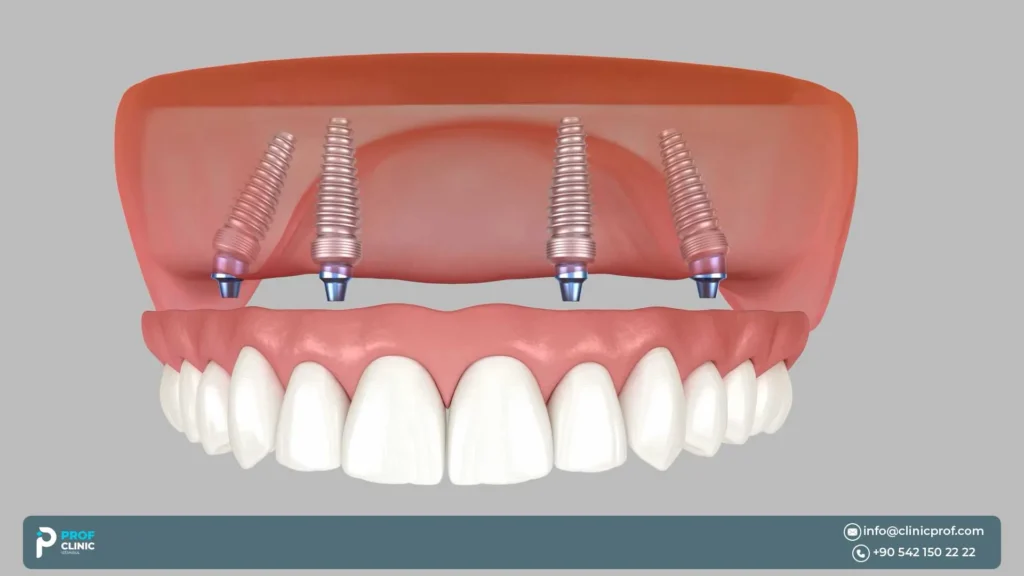
Does the upper jaw require tilted implants?
Not always, but tilted posterior implants are common in the upper jaw. They’re often used to avoid the maxillary sinus and improve implant spread/support for the bridge. The exact angle and need for tilting depend on your CBCT anatomy and the prosthetic plan.
Can All-on-4… without bone grafting?
Sometimes. All-on-4 was designed to reduce the need for grafting by using stronger anterior bone and angling posterior implants—so “graftless” is realistic in many cases. But if bone volume is severely reduced or sinus anatomy is unfavorable, you may still need sinus lift/grafting, more implants, or an advanced option (like zygomatic implants).
Sources
- The all-on-four treatment concept: Systematic review
- All-on-four concept… longitudinal study with 3–17-year follow-up
- Sinus membrane elevation and implant placement
- Maxillary sinus lift procedures: overview, evaluation, complications
- CBCT assessment for dental implant surgery at the maxilla
- ITI consensus report on zygomatic implants
- Success rates of zygomatic implants
- Prevention and management of intra-operative complications in maxillary sinus augmentation