If you’ve been told you have severe upper jaw bone loss, failed implants, or not enough bone for a fixed bridge, and you want an option that may avoid major grafting, this guide on all on 4 zygomatic implants
is for you.
This article by Prof Clinic Istanbul is for education only and can’t replace an in-person exam. A safe plan for complex full-arch cases typically depends on CBCT, bite analysis, and medical clearance
What does All-on-4 with Zygomatic Implants Mean?
When people search all on 4 zygomatic implants, they’re usually trying to understand a confusing phrase that clinics use in different ways.
Here’s the simplest, most accurate way to think about it:
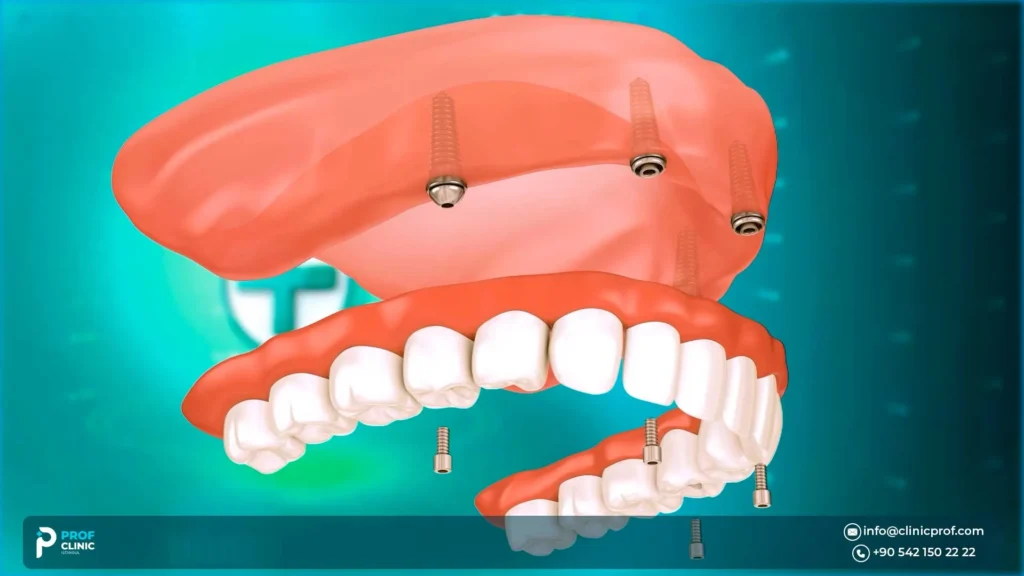
- Classic All-on-4 is a full-arch concept where a fixed bridge is supported by four implants, often with angled posterior implants when anatomy allows.
- Zygomatic implants are longer implants anchored into the zygoma (cheekbone) to support upper-arch restoration when the upper jawbone is too thin or the sinus anatomy limits conventional implants.
- In real life, All-on-4 with zygomatic implants often describes a hybrid full-arch design. The exact design is determined after CBCT planning and prosthetic bridge analysis.
Also read: Zygomatic Implants Turkey: Solution for Severe Bone Loss
What are zygomatic implants in All-on-4?
They’re advanced anchoring implants used mainly in the upper jaw when the bone is severely resorbed. Instead of relying on weak posterior maxillary bone, often near the sinus, they gain stability by engaging denser bone and/or alternative anatomy—commonly the zygoma, so a fixed full-arch bridge becomes feasible in cases that might otherwise require major bone reconstruction.
What factors make zygomatic implants different from regular dental implants?
Key differences:
- Length & path: Zygomatic implants are typically longer and follow a different trajectory than standard implants.
- Anatomy & complexity: They’re placed near sensitive structures, so they require specialized surgical training and planning.
- Prosthetic implications: Because the anchor point and angulation can differ, the bridge design, hygiene access, and load distribution must be planned carefully to reduce complications.
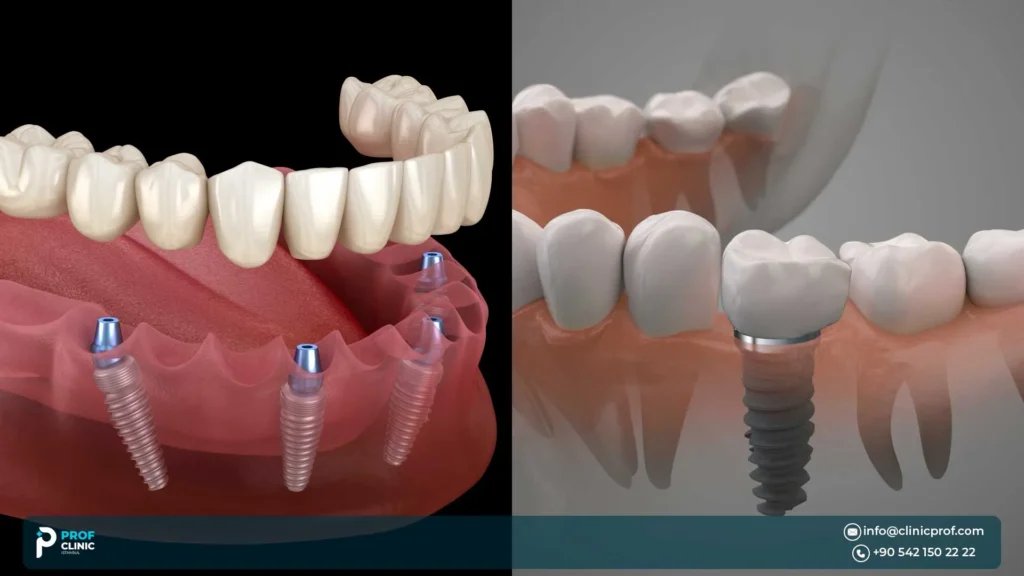
Traditional implants vs. zygomatic implants
- Traditional implants typically anchor in the alveolar bone (the jaw ridge where teeth used to be).
- Zygomatic implants are chosen when that ridge is inadequate, especially in the upper jaw, so the plan shifts to using an alternative anchor that can support a fixed full-arch restoration.
In other words, it’s not better implants; it’s a different solution for a different anatomy problem.
How can zygomatic implants eliminate the need for bone grafting
The phrase no bone graft is often used loosely. A safer, more accurate statement is:
In selected severe upper-jaw bone-loss cases, a zygomatic or hybrid full-arch plan may reduce or avoid major bone grafting, but only after CBCT-based evaluation confirms a safe pathway and adequate stability.
How do zygomatic implants eliminate the need for bone grafting?
They work by changing the anchorage strategy:
- Instead of trying to rebuild the upper jaw ridge with grafts first, the plan may use existing stable anatomy for anchorage.
- This can bypass the typical “graft, heal, implant” sequence, which in many grafting scenarios can take a prolonged healing period before implants and final teeth are completed.
- For moderate bone loss, conventional implants plus sinus lift/augmentation may still be appropriate, so the goal is not “avoid grafting at all costs,” but “choose the safest pathway for your anatomy.
If you’re trying to avoid grafting, the quickest reality-check is a CBCT feasibility review. Book a free online consultation to discuss your case and help you to do the necessary.
Also read: Full Arch Dental Implants: Restoring a Complete Smile
Zygomatic All-on-4 vs Classic All-on-4 vs Bone Grafting
What is the difference between All-on-4 and zygomatic All-on-4?
- All-on-4 (classic): four conventional implants (upper or lower) support a fixed bridge when adequate bone and safe angulation are available.
- Zygomatic All-on-4: a label often used for an upper full-arch plan that includes zygomatic implants (sometimes alongside All-in-clusive dental implants). The “4” does not guarantee a fixed formula. Some cases need different counts or hybrid distributions depending on anatomy and bite forces.
Are zygomatic implants better than bone grafting?
It depends on your case. A balanced way to decide:
- Zygomatic or hybrid graftless designs can be a strong alternative when the upper jaw is extremely atrophic, especially when major grafting would be extensive, staged, or uncertain.
- Bone grafting can be appropriate when the defect is moderate and predictable, and when staged healing fits the patient’s health, timeline, and goals.
- The best plan is the one that matches your anatomy, sinus status, bite, medical risks, and your ability to maintain the bridge long-term.
How many zygomatic implants are needed for full-arch restoration?
There isn’t one universal number. Common real-world patterns include:
- Hybrid: one or two zygomatic implants plus conventional implants in the front when front bone is usable.
- More zygomatic support: in extreme atrophy, designs may require more reliance on zygomatic anchorage.
- Alternatives/adjuncts: some cases use other posterior anchorage concepts to optimize support and load distribution.
Your CBCT findings bone volume, sinus anatomy), infection history, and prosthetic design constraints determine the safest distribution.
Bone grafting vs Classic All-on-4 vs Zygomatic All-on-4
| Pathway | Best for | Need for graft | Typical implants used | Timeline concept | Key risks to discuss | Maintenance reality |
| Bone graft and conventional implants | Moderate–severe bone loss where reconstruction is feasible | Often yes (case-dependent) | Conventional implants after augmentation | Often staged; healing can be prolonged | Graft healing variability, infection risk, multiple surgeries | Similar bridge hygiene demands; longer overall journey |
| Classic All-on-4 | Patients with adequate bone and safe angulation | Sometimes no, sometimes yes | Four conventional implants supporting a fixed bridge | May allow faster restoration when stability is strong; final teeth often later | Immediate-load risk if stability is borderline; prosthetic complications | Daily under-bridge cleaning; periodic professional checks |
| All on 4 zygomatic implants | Extreme upper jaw atrophy or anatomy limiting conventional posterior implants | Often reduced major grafting in selected cases | Zygomatic implants ± anterior conventional implants | May shorten the “graft-first” pathway; final teeth still depend on healing | Sinus-related issues, infection, sensory changes, prosthetic load problems | Meticulous hygiene + follow-up are non-negotiable; repairs/relines may occur |
Who is a candidate for zygomatic All-on-4?
Who is a candidate for All-on-4 with zygomatic implants?
You may be a candidate if you have one or more of the following:
- Severe upper jaw bone loss: Long-term denture wear, long-standing missing teeth, and advanced resorption.
- Failed grafts or failed conventional implants: In the upper jaw after root-cause analysis.
- Sinus anatomy that limits conventional posterior implant placement (requires careful evaluation, not assumptions).
Are zygomatic implants suitable for severe bone loss?
That’s the primary indication discussed in the literature: extreme maxillary atrophy is the most commonly cited indication, though definitions of “extreme” vary across studies—another reason imaging-based planning matters.
Pay attention to these red flags:
- Uncontrolled systemic disease affecting healing, immunosuppression (case-by-case).
- Active infection/untreated periodontal disease.
- Heavy smoking or uncontrolled bruxism without a mitigation plan.
- Known sinus disease or symptoms that may require ENT co-management before/after surgery.
If you want to confirm whether you likely need zygomatic, pterygoid/hybrid, or classic All-on-4, the most useful first step is an evaluation request and then a CBCT-based plan discussion. Prof Clinic offers a consultation request form for international patients. Book an appointment today

How Doctors Evaluate Bone for Zygomatic Implants
Complex upper-arch cases should feel process-driven, not sales-driven. A credible clinic, like Prof Clinic in Turkey, should be able to explain how they decide your implant distribution and why.
A safe evaluation commonly includes:
- CBCT: assesses bone volume, sinus anatomy, and spatial relationships for planning. Professional guidance in implant dentistry emphasizes the value of cross-sectional imaging (CBCT) for implant assessment and planning.
- Prosthetic-driven planning: the bridge design and bite forces influence implant position, angulation, and load distribution.
- Sinus assessment: Your risk profile changes if there’s existing sinus disease, thickened mucosa, prior sinus surgery, or chronic symptoms. This is where ENT input may be appropriate.
- Risk factor review: Smoking, hygiene capacity, diabetes control, and bruxism management plan.
Can zygomatic implants be done after failed traditional implants?
Often, yes, but only after root-cause analysis, such as:
- Was there infection around the old implants?
- Was the bite overload (grinding, poor load distribution, cantilever issues)?
- Was hygiene impossible due to bridge design?
- Were there systemic factors or smoking that weren’t controlled?
A redo case should come with a clear prevention plan because repeating the same risks can repeat the same failure.
Questions to ask your clinic
- Will you review my case using CBCT, and will you explain the sinus findings?
- What’s the proposed design: classic All-on-4, hybrid, or other? Why?
- What happens if primary stability is not ideal—do you stage the case or change the plan?
- What is your follow-up plan once I return home (remote check-ins, local dentist coordination)?
- How do you design the bridge for hygiene access and long-term maintenance?
Visit our medical team page to learn more about their experiences

The Procedure in Istanbul: Surgery, Teeth Timing, and Full-Arch Prosthetic Design
Here’s where expectations can get distorted online, especially around same-day teeth.
Depending on your case complexity, anxiety level, and medical clearance, implant surgeries can be done with local anesthesia, sometimes with sedation. At Prof Clinic, our clinician explains options and risks in writing for your situation.
Teeth timing
- Many full-arch workflows aim for a temporary fixed bridge relatively quickly when stability and infection control allow.
- Final teeth are typically delivered after a healing phase, once integration and soft-tissue stability support a more definitive prosthetic.
What the bridge is like
- You’ll need to learn cleaning “under” the bridge (water flosser, superfloss, interdental tools).
- Speech may feel different at first (especially “s” sounds); adjustments are common.
- Follow-up visits (or remote check-ins) matter—bite refinements and hygiene coaching reduce complications.
The final number can change after CBCT, bite assessment, and surgical stability checks.
Safety, Risks, and Sinus Questions about All on 4 Zygomatic Implants
Is All-on-4 with zygomatic implants safe?
It can be safe in appropriately selected patients with thorough planning and experienced surgical/prosthetic execution. The literature discussing zygomatic implants repeatedly highlights that complication profiles exist, especially sinus-related and that standardized complication reporting and careful management are important.
What are the risks or complications of zygomatic implants?
Rather than quoting “success rates” out of context, here are risk categories you should discuss clearly:
Common-to-possible
- Swelling, bruising, temporary discomfort (expected after surgery)
- Prosthetic adjustments (bite refinements, sore spots, minor repairs)
Important
- Sinus-related complications: Sinusitis is frequently discussed as a key complication topic in zygomatic implant literature
- Infection risk, especially if prior infection existed,
- Sensory changes/numbness (often temporary, sometimes longer)
Less common but serious
- Significant sinus pathology requiring ENT co-management
- Implant integration failure (risk varies by case and risk factors)
Risk reducers (what credible clinics do):
- CBCT-based pathway planning + sinus assessment
- A “plan B” if stability/infection control isn’t ideal (staged approach, modified loading)
- Prosthetic design that reduces overload and allows hygiene access
- Structured follow-up and maintenance plan
Do zygomatic implants affect the sinuses?
They can, because the upper jaw and zygomatic pathways are anatomically close to the sinus region, and sinus complications are one of the most discussed issues in the complication literature. That doesn’t mean problems are inevitable—but it does mean you should expect your clinician to:
- Review sinus health on CBCT,
- Ask about chronic sinus symptoms, and
- Coordinate ENT care when indicated.
If a clinic won’t explain sinus findings, temporary vs final teeth, and the complication plan in writing, consider that a red flag. Our All-on-4 guidance emphasizes protocol checks like CBCT planning and clear aftercare planning

Zygomatic Full-Arch Recovery in Turkey: Aftercare and Next Steps
For international patients having zygomatic full-arch treatment in Turkey, recovery planning also affects hotel stay, follow-up timing, and when it is safe to travel home.
Recovery
- Expect swelling and soreness early; improvement is gradual.
- Bone healing/integration is measured in months, even if you receive functional temporary teeth sooner.
- If grafting is part of your plan, healing can extend longer; dental bone graft timelines vary and can be prolonged in some cases.
Aftercare basics
- Soft diet as advised; avoid overload while healing
- Daily under-bridge cleaning routine (this is non-negotiable)
- Professional maintenance visits (locally or at your treating clinic)
- Nightguard if you clench/grind (bruxism management is a common “make-or-break” factor)
Travel planning
- You may need more than one touchpoint: initial procedure and follow-up checks and/or final prosthetic delivery timing, depending on your plan.
- Choose a clinic that offers a clear pathway for international patients: remote review, in-clinic confirmation, and aftercare plan.
- At Prof Clinic in Istanbul, we describe consultation requests and case review steps for international patients.
Post-op packing list (simple but useful):
- Prescribed meds and written instructions
- Soft-food options for the first days
- Water flosser or plan to buy locally and superfloss/interdental brushes
- Your CBCT copy (digital) and treatment plan document
- Emergency contact route for your clinic
All on 4 zygomatic implants can be a powerful zygomatic full arch pathway for people with severe upper jaw bone loss, especially when the goal is to potentially avoid extensive grafting. The safest shortcut is not a slogan; it’s a CBCT-based plan, sinus assessment, and a written roadmap that separates temporary fixed teeth from final teeth expectations. You can also visit our All-Inclusive Dental Package
If you want a clear, itemized treatment roadmap, request a consultation and case review through our booking pathway.
FAQs about all on 4 zygomatic implants
What is the success rate of zygomatic implants?
Reported outcomes vary by anatomy, sinus health, surgical/prosthetic experience, and maintenance. Because complication reporting differs across studies, the safest interpretation is your personalized risk profile after CBCT review and medical screening.
How long do zygomatic implants last?
They’re designed for long-term function, but longevity depends on hygiene, smoking status, bite forces (clenching), medical factors, and regular professional follow-up and prosthetic maintenance.
Is the procedure painful?
You typically won’t feel pain during surgery due to anesthesia, but afterward swelling and soreness are common. Your clinician should provide a clear pain-control and aftercare plan tailored to your health history.
What is the recovery time after zygomatic All-on-4?
Early recovery is often days to a couple of weeks for swelling and soreness, while full integration/healing and final-teeth timing are usually measured in months. A reputable clinic should outline temporary vs final milestones in writing.
Can I get teeth the same day with zygomatic implants?
In some cases, a temporary fixed bridge can be delivered quickly when stability and infection control allow. Whether that’s appropriate depends on CBCT findings, surgical stability, and the loading plan.
How Much Do All-on-4 Zygomatic Implants Cost in Turkey?
Cost depends on the implant design (hybrid vs more zygomatic support), anesthesia needs, extractions, prosthetic materials, imaging, and follow-up care. The fairest way to compare clinics is to request an itemized written plan after imaging review.
Sources
- extreme maxillary atrophy as a main indication.
- zygomatic implants as an alternative to major grafting in selected severe cases.
- Complications of zygomatic implants (clinical series / review,
- Surgical complications in zygomatic implants
- Maxillary sinusitis after zygomatic implants (literature review)
- Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography
- Cone beam computed tomography in implant dentistry: recommendations for clinical use
- Healing Process for Dental Implants