If you’re researching all on 4 vs all on 6, you’re likely trying to balance three things: long-term reliability, how much bone you have, and what fits your budget and timeline. Both options can replace a full arch of teeth with a fixed (non-removable) bridge—often with the possibility of leaving the clinic with temporary fixed teeth when conditions allow.
For patients planning full-arch implant treatment in Turkey, the difference between All-on-4 and All-on-6 affects not only stability, but also cost, timeline, and whether grafting may be needed. The fastest way to narrow the choice is to review a CBCT scan + bite forces + medical history with an implant dentist. Ask for a written plan that explains why 4 or 6 implants are recommended for your jaw.
This article is for education and does not replace an in-person diagnosis. Implant treatment must be planned by a qualified dental professional after imaging and a full medical/dental exam.
Understanding All-on-X full-arch implants
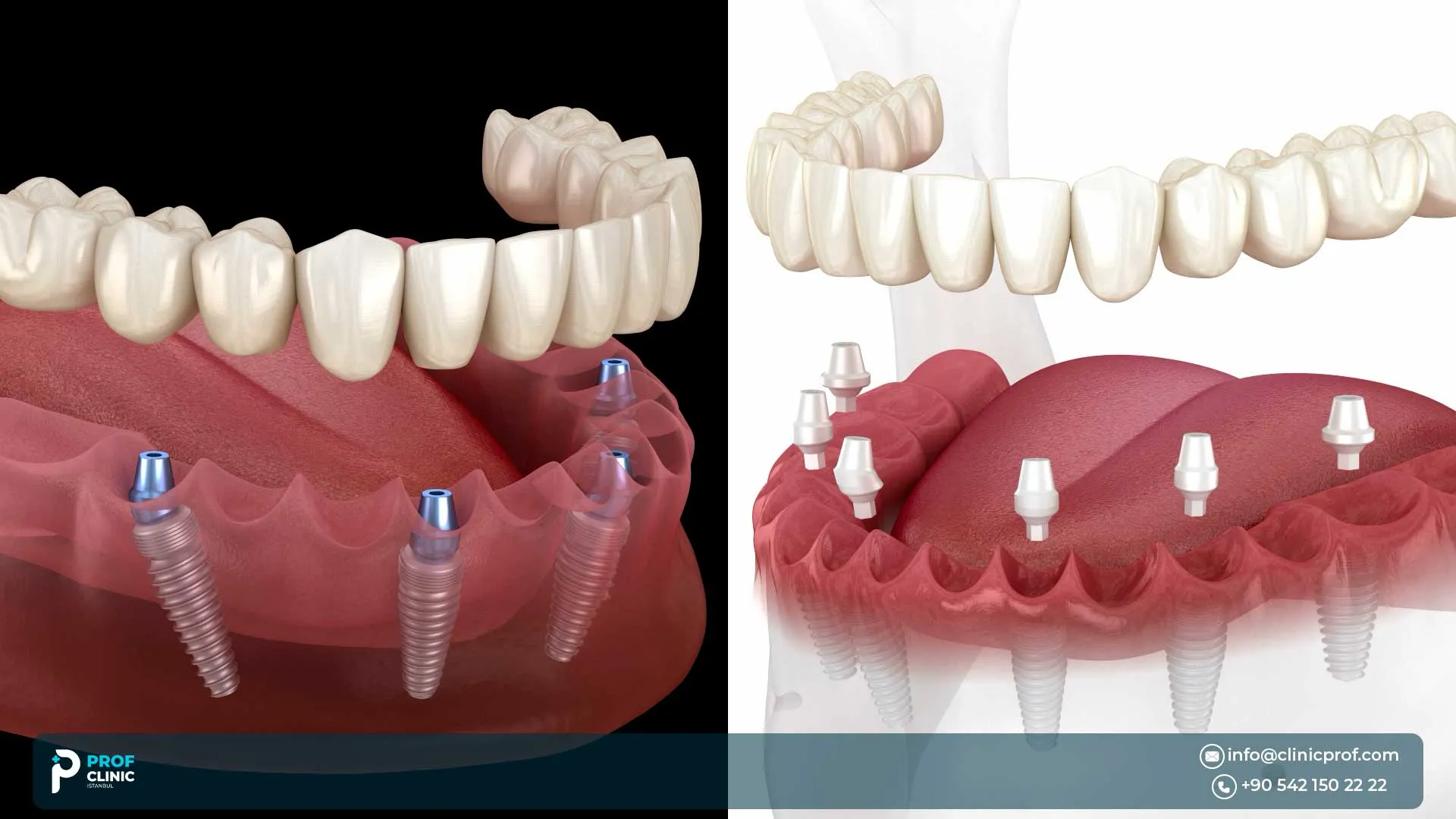
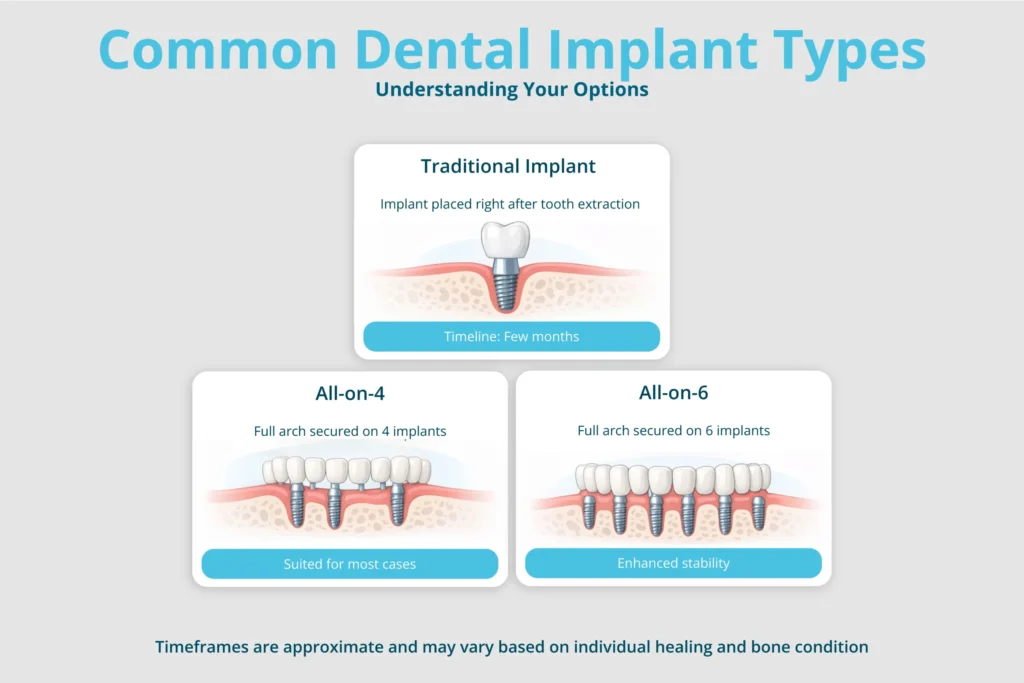
“All-on-4” and “All-on-6” are full-arch rehabilitation concepts: a complete set of upper or lower teeth is supported by 4 or 6 implants placed strategically in the jaw. The prosthesis is typically a fixed bridge.
Implant number is only one part of the plan. Implant position, bone quality, arch shape, bite force (and habits like clenching), and prosthetic material often matter just as much.
All on 4 vs all on 6
Here’s a practical, patient-focused 4 vs 6 implants comparison to guide your next questions.
| Factor | All-on-4 | All-on-6 |
| Implants per arch | 4 implants | 6 implants |
| Common design | 2 front implants and 2 back implants often angled | 6 implants spread across the arch (often axial/straight, sometimes mixed) |
| Typical goal | Efficient full-arch support with fewer implants | More “distribution points” for load sharing |
| Bone strategy | Often designed to use available bone and may help avoid grafting in select cases (case-dependent) | May require adequate bone in more sites; sometimes still graftless, sometimes not |
| Stability & load | Very good outcomes when planned correctly; cantilever length and bite forces matter | Often chosen when clinicians want more support/distribution, especially for higher forces or design preferences |
| Implant survival | High survival reported in studies; direct comparisons often show similar mid-term survival | Direct comparisons also show high survival; some studies suggest differences may appear in certain subgroups |
| Cost drivers | Fewer implants may reduce surgical and component costs | More implants and components can increase cost |
Direct comparative research in a large cohort found high, comparable 2- and 5-year implant survival for four- vs six-implant full-arch fixed restorations under a systematic treatment protocol.
How All-on-4 works and why implants are often tilted?
All-on-4 commonly uses two straight anterior implants and two posterior implants tilted up to ~45°. The purpose of tilting is not “magic”—it’s biomechanics and anatomy:
- It can help avoid vital structures (maxillary sinus in the upper jaw, nerve canal in the lower jaw).
- It can improve the antero-posterior spread, often reducing the need for long cantilevers (the “overhang” behind the last implant).
- In some patients, it can reduce the need for bone grafting, though this is not guaranteed and depends on bone volume/quality and the plan.
Many All-on-4 workflows are designed for immediate function (temporary fixed teeth soon after surgery) when criteria are met, including adequate implant stability.
Also read: Same-Day All-on-4: Teeth in One Day Possible?
How All-on-6 works and what changes with two extra implants
All-on-6 uses six implants to support a full arch. The main advantage is simple: more implants can mean more support points, potentially:
- distributing load over a larger area,
- offering more prosthetic design flexibility,
- providing a bit more “insurance” if one implant develops problems in the future, depending on prosthesis design.
But reality check: more implants also mean more components, more surgical sites, and sometimes higher cost and complexity.
Also read: All-on-6 Dental Implants: More Stability Explained
Which all on type better for stability?
People often ask which all on better for stability. The most accurate answer is: stability is case-specific, but here are the levers that matter most:
1) Bone quality and implant anchorage
Upper jaws often have different bone characteristics than lower jaws, which can influence implant planning and risk profiles.
2) Cantilever length and bite forces
Longer cantilevers can increase stress on implants and prosthetic screws/materials. Some biomechanical studies show stress differences between configurations (often favoring more distributed designs), but these are models—not your personal biology.
3) What real-world comparative data suggests
A large retrospective comparison found very similar 2- and 5-year implant survival between four- and six-implant full-arch fixed restorations overall.
Another clinical study reviewing long-term outcomes reported no major overall difference between groups, while noting that differences may appear in certain clinical characteristics and clinician preferences.
If you have strong bite forces, a history of fractures/loosened dental work, or bruxism (clenching/grinding), your dentist may lean toward designs that reduce cantilever stress and/or add support—sometimes that means All-on-6, sometimes it means different implant distribution/material choices.
Is All-on-6 more durable than All-on-4?
Durability has two layers:
- Implant survival: The implants stay integrated in bone.
- Prosthesis durability: The bridge stays intact and comfortable—minimal chipping, fractures, screw loosening, etc.
Implant survival in both concepts is generally high in published studies, and at least one large cohort comparison found comparable mid-term survival between four and six implants.
However, many long-term patient frustrations come from maintenance issues. Reviews of full-arch restorations commonly describe technical complications such as material chipping/fracture and other prosthetic issues over time—so material choice and maintenance planning matter a lot.
Also read: Fixed vs Removable Implant Dentures: Pros & Cons

Who is a good candidate for All-on-4 implants?
All-on-4 is often considered when a patient wants a fixed full-arch solution with fewer implants and the anatomy allows strategic placement—sometimes using tilted posterior implants to work around the sinus/nerve and available bone.
Common candidate patterns must be confirmed with imaging:
- Controlled medical risks
- Adequate bone in key anchorage areas
- Good oral hygiene capability and commitment to follow-ups
- Willingness to follow a soft-diet and aftercare plan during healing
- Fully edentulous (no teeth) or “failing teeth” planned for extraction
Smokers and older patients: special considerations
Smoking
A systematic review/meta-analysis found implants placed in smokers had a significantly higher failure risk (reported as ~2.4× odds), and the effect persisted across time; it also reported higher marginal bone loss in smokers.
This doesn’t mean smokers can’t get implants, but it does mean the plan should include risk reduction and realistic expectations.
Age
Older age alone doesn’t automatically disqualify you; overall health, medications, bone status, and hygiene capability matter more than a number on your passport
Who should consider All-on-6 instead of All-on-4?
All-on-6 may be considered when the clinical team wants:
- More support points for load distribution,
- More flexibility in prosthetic design (e.g., reducing cantilever),
- Added planning “margin” in specific risk profiles.

Upper jaw vs lower jaw: which option is better?
This is a huge decision point.
- Upper jaw: Anatomy (sinus) and bone quality can influence placement and stability. Some comparative data show survival remains high in both approaches, with differences sometimes more noticeable in maxillary sub-analyses.
- Lower jaw: Anatomy (nerve canal) and typically different bone density patterns can change the plan. In the same cohort, mandibular survival rates were high across both groups.
It’s not “All-on-4 is for lower, All-on-6 is for upper.” At Prof Clinic in Turkey, we use either, based on ridge shape, bone volume, sinus/nerve location, and bite forces. Book an appointment with our team and let’s discuss your case.
Does All-on-6 require more bone density than All-on-4?
Often, yes in planning terms because you’re placing two additional implants, you need acceptable bone in more sites, or you need a plan to create bone with grafting. But there are exceptions: surgeons may place implants in different positions, or use angled/tilted strategies, depending on anatomy.
Bone requirements are determined by CBCT findings, implant length/diameter options, and whether grafting is planned, not by the label alone.
Is bone grafting needed for All-on-4 or All-on-6?
Bone grafting is sometimes needed for either option. All-on-4 was developed to maximize available bone in atrophic jaws and may help avoid regenerative procedures in selected cases.
If grafting is needed, it can extend the timeline, especially for larger grafts, which may require months of healing before implants can be placed or loaded.
Start with a free online consultation to show you, on your CBCT scan, whether the plan is graftless or grafted and how that changes timeline, risk, and cost.
Also read: Basal Implants: Immediate Loading Without Bone Graft
Can All-on-4 or All-on-6 be done in one day?
In many clinics, patients can receive fixed provisional teeth on the day of surgery if they meet immediate-loading criteria and adequate stability is achieved.
Keep in mind that “Teeth in a day” usually means temporary fixed teeth first, followed later by a definitive prosthesis after healing.
Is the procedure painful in both implant types?
During surgery, you should not feel pain due to local anesthesia; sedation options may be available depending on the clinic and your needs. After surgery, discomfort and swelling are common for a short period.
How Long Does Recovery Take for All-on-4 vs All-on-6 in Istanbul?
Recovery has two tracks:
- Short-term surgical recovery (days to a couple of weeks): swelling, soreness, adapting to temporary teeth and diet.
- Biologic integration (months): the bone stabilizes around the implants while you transition to the final prosthesis.
Post-op aftercare guidance commonly notes swelling can peak around the first couple of days and then gradually settle (exact pattern varies).
All-on-4 vs All-on-6
Many patients experience similar recovery patterns; All-on-6 may involve more surgical sites, which can affect swelling for some people, but technique, extractions, grafting, and sedation type often dominate the recovery experience.
Also read: Types of Dental Implants: Complete Guide 2026

Do All-on-4 and All-on-6 look natural and feel like real teeth?
They can look very natural, especially when the prosthesis is designed with proper lip support, tooth shape, smile line, and gum architecture. Your feel depends on:
- speech adaptation,
- how your bite is adjusted,
- prosthesis material and thickness,
- how well the prosthesis fits and is cleaned.
A well-designed fixed full-arch restoration is typically far more stable than removable dentures and often improves confidence in speaking and chewing.
Maintenance and cleaning: 4 vs 6 implants comparison
Many long-term failures are not implant rejection; they’re inflammation and preventable complications linked to hygiene and risk factors.
Recent consensus and expert guidance emphasize prevention, risk-factor control, and supportive peri-implant care as essential for long-term peri-implant health.
At home, cleaning often includes:
- a soft toothbrush + low-abrasive toothpaste,
- interdental tools designed for implants/bridges
- antimicrobial rinses only if prescribed,
- avoiding smoking
What happens if one implant fails in All-on-4 or All-on-6?
This is one of the most important questions.
- With All-on-4, losing one implant can be more disruptive because you have fewer supportsو sometimes requiring revision surgery, adding an implant, or redesigning the prosthesis.
- With All-on-6, there may be more redundancy, but it depends on how the prosthesis is designed and where the failure occurs.

All-on-4 vs All-on-6 Cost Difference in Turkey: What Actually Drives the Price?
Instead of giving misleading average prices, here’s what typically changes the quote:
| Cost driver | Why it matters |
| Number of implants | More implants = more components and surgical time |
| Extractions & infection control | Removing failing teeth and treating infection can add steps |
| Bone grafting / sinus-related procedures | Can add materials, time, and healing phases |
| Provisional teeth (same-day) | Lab work and materials add cost |
| Final prosthesis material | Acrylic/resin vs zirconia/ceramic options affect cost and repair patterns |
| Guided surgery | May increase planning cost but can improve workflow |
| sedation type | Deeper sedation usually costs more |
| Follow-up and maintenance program | Long-term outcomes rely on professional maintenance |
Ask for an itemized plan by scheduling a meeting, so you can compare offers fairly.
How Do I Choose Between All-on-4 and All-on-6 in Turkey?
If you’re comparing full-arch treatment options in Turkey, this decision should balance bone anatomy, maintenance needs, recovery logistics, and long-term prosthetic stability.
Use this checklist in your consultation:
- CBCT reality: Do you have enough bone for 6 implants without grafting? If not, is grafting acceptable to you (timeline/cost)?
- Bite force & habits: Do you clench/grind? Any history of broken crowns/bridges?
- Jaw-specific anatomy: Sinus position (upper), nerve canal (lower), arch shape.
- Prosthesis design: How long is the cantilever? What material is planned, and what are typical complications?
- Risk factors: Smoking, periodontal history, diabetes control—what is your risk-reduction plan?
- Maintenance commitment: Are you ready for ongoing supportive care visits and home hygiene?
At Prof Clinic, we can explain these points clearly with your scan on the screen; you’re in the right place. Book an appointment now!
FAQs about all on 4 vs all on 6
What is the difference between All-on-4 and All-on-6 dental implants?
All-on-4 uses four implants to support a full-arch fixed bridge, while All-on-6 uses six implants. The real difference isn’t only the number. It’s also implant distribution, prosthesis design, and cantilever length, which affect load sharing and maintenance needs. Your bone anatomy (from a CBCT scan) usually determines which concept fits best.
Which option provides better stability, All-on-4 or All-on-6?
Both can be very stable when planned correctly. All-on-6 may offer more load distribution (more support points), which can be helpful for higher bite forces or certain arch designs. But many patients do extremely well with All-on-4—stability depends more on bone quality, implant position, and bite design than on implant count alone.
Who should consider All-on-6 instead of All-on-4?
All-on-6 may be preferred if you have strong bite forces, a wider arch that benefits from more support points, or if your dentist wants to reduce stress on the bridge by distributing forces across more implants. It can also be chosen when the plan aims to minimize cantilever length or increase design flexibility. The best choice depends on your jaw anatomy and prosthetic plan.
What is the cost difference between All-on-4 and All-on-6?
All-on-6 is often more expensive because it uses more implants and components, and may involve more surgical and lab work. However, total cost is mainly driven by factors like bone grafting, extractions, sedation type, temporary teeth, and final bridge material—not just “4 vs 6.”
How long does the recovery take for each option?
Short-term recovery (swelling, tenderness) is usually days to about 1–2 weeks, depending on extractions and surgical complexity. Full healing and stabilization for the final prosthesis often takes months, especially if grafting is involved. Many patients return to normal daily activities relatively quickly, but diet and aftercare instructions are crucial.
Is bone grafting needed for All-on-4 or All-on-6?
Sometimes, for either option. All-on-4 may reduce the need for grafting in certain cases by using strategic implant placement, but it’s not guaranteed. Whether grafting is needed depends on bone volume, bone quality, and implant positions seen on your CBCT scan.
Which option is better for patients with severe bone loss?
There’s no universal winner. Some severe bone-loss cases can be treated with graftless strategies and careful implant positioning, while others may require bone grafting or advanced implant approaches. The “better” option is the one that gives a safe, stable plan based on your anatomy and risk factors.
Is sedation available during All-on-4 and All-on-6 procedures?
Often yes, depending on the clinic and your medical suitability. Options may include local anesthesia, oral sedation, IV sedation, or sometimes general anesthesia. Your dentist will recommend what’s safest based on your anxiety level, medical history, and treatment complexity.
How do I choose between All-on-4 and All-on-6?
Choose based on your CBCT scan findings, bone quality/volume, bite forces (especially if you grind or clench), and the prosthesis design (cantilever length, materials, maintenance plan). Ask your provider to explain the plan on your scan and compare both options with clear reasoning. The “right” choice is the one that best balances stability, risk, maintenance, and cost for your specific case.
Additional sources
- The all-on-four treatment concept: Systematic review
- Number of Implants Placed for Complete-Arch Fixed Prostheses
- Comparison between all-on-four and all-on-six treatment concepts on stress distribution for full-mouth rehabilitation using three-dimensional finite element analysis: A biomechanical study
- Comparison of 4- or 6-implant supported immediate full-arch fixed prostheses: A retrospective cohort study of 217 patients followed up for 3-13 years
- Four vs. Six Implant Full-Arch Restorations—A Direct Comparative Retrospective Analysis in a Large Controlled Treatment Cohort
- Fixed Full-Arch Implant-Supported Restorations: Techniques Review and Proposal for Improvement
- Outcomes of Peri-Implantitis Treatment Followed by Supportive Care
- Smoking and Dental Implants: A Systematic Review and Meta-Analysis